Bone marrow collection adds an invasive procedure before regenerative treatment can even begin. Umbilical cord-derived cells remove that harvesting step, but the right choice still depends on your health, goals, and treatment plan.
Schedule a Free Stem Cell Consultation ->
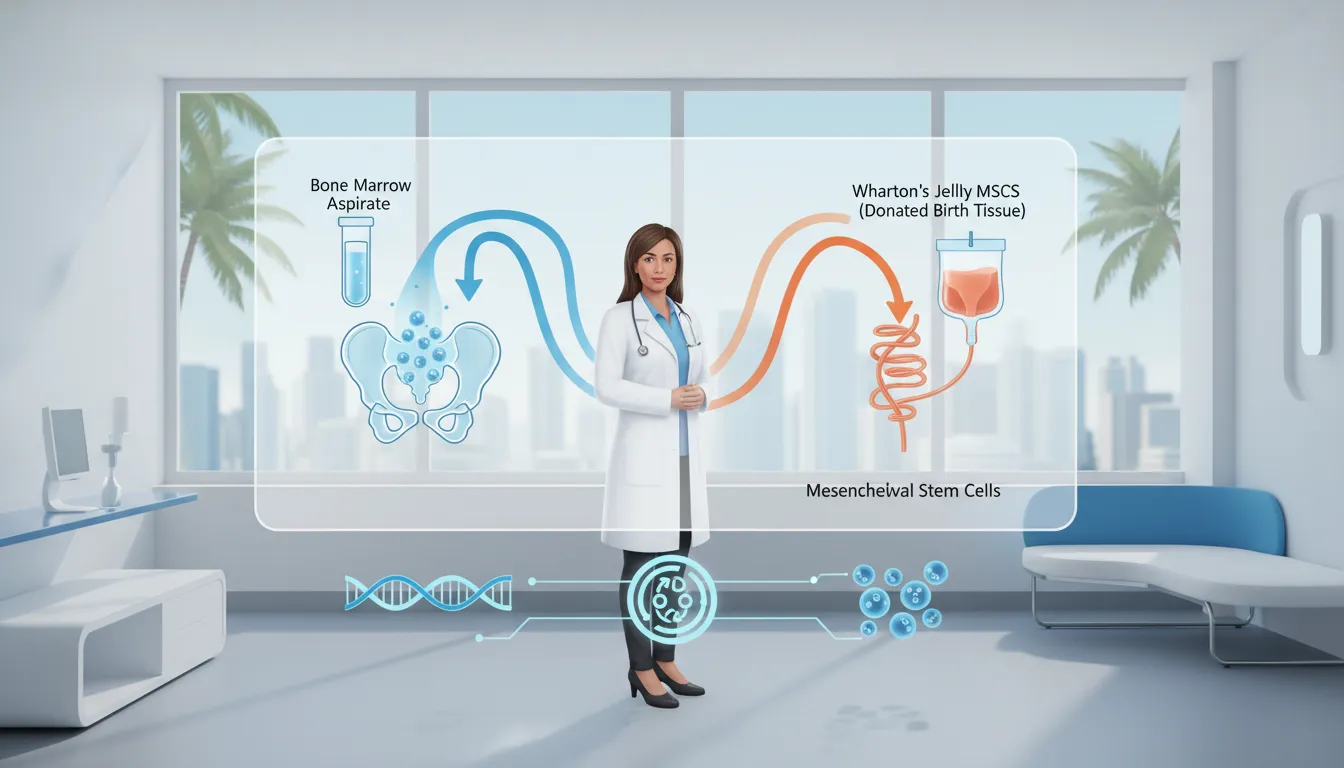
Bone marrow aspirate vs umbilical cord stem cells is primarily a choice between autologous cells collected from your pelvis and donor-derived cells obtained after birth. Bone marrow aspiration usually requires anesthesia and creates a second recovery site, while umbilical cord MSCs do not require harvesting from the patient. Marrow cell quality and yield can vary with age; research comparing MSC sources found cord blood MSCs had higher proliferation and clonality. This difference may matter for older patients, because cells collected from their own marrow reflect age and individual health. Neither source is automatically right for every person; a qualified provider should assess diagnosis, goals, product quality, safety, and available clinical evidence.
The practical question is not simply which source sounds newer, but which procedure and biological profile fit your needs in real treatment decisions. Before comparing possible uses, safety, and recovery, start with Bone marrow aspirate vs umbilical cord stem cells: the core difference. Here’s how.
Bone marrow aspirate vs umbilical cord stem cells: the core difference
The core difference is where the cells come from and how they reach the treatment setting. Bone marrow aspirate comes from the patient’s own marrow. Umbilical-cord-derived mesenchymal stem cells, or MSCs, come from donated tissue collected after birth.
This source difference shapes collection, preparation, and the patient experience. It does not prove that one option is best for every person or condition. Research shows that MSCs from several tissues share key traits, yet their growth patterns can differ. One study found higher proliferation and clonality in cord-blood-derived MSCs than in adult bone-marrow-derived MSCs.
Source and collection
Bone marrow aspirate is collected directly from the patient, often from the pelvis. The sample is then processed into bone marrow aspirate concentrate, commonly called BMAC. This approach requires a separate marrow collection procedure before the prepared material can be used.
Umbilical cord tissue is collected after a healthy birth, rather than taken from the person receiving treatment. The tissue can serve as a readily available cell source. A scientific review of umbilical cord stem cells describes several postnatal cord sources, including cord blood, vein, and matrix cells.
| Point. | Bone marrow aspirate. | Umbilical-cord-derived MSCs. |
|---|---|---|
| Cell source. | Patient’s own bone marrow. | Donated postnatal cord tissue. |
| Source type. | Autologous. | Allogeneic. |
| Collection. | Marrow aspiration from the patient. | Collected after birth from a donor. |
| Patient procedure. | Includes marrow harvesting. | No marrow harvest from the recipient. |
| Source variability. | Linked to the patient’s marrow. | Prepared from screened donor material. |
Autologous and allogeneic sources
Autologous means the material comes from the same patient who receives it. Allogeneic means the source is another donor. These terms describe the source relationship, not a promise about safety, potency, or results.
Source biology also deserves careful review. In laboratory research, cord-blood-derived MSCs showed higher cell growth and lower expression of several aging markers than adult bone-marrow MSCs. The published comparison of MSC sources also found similar surface markers and differentiation ability across the tested tissues.
Why this is not a transplant comparison
This article compares regenerative procedures, not bone marrow transplantation with cord blood transplantation. Transplants are separate medical treatments used in different care settings. They involve distinct goals, patient selection, risks, and clinical steps.
That distinction keeps the decision focused on the actual procedure a patient may face. With BMAC, the process includes harvesting and preparing the patient’s marrow. With cord-derived products, the recipient does not undergo marrow collection. Readers can explore umbilical cord stem cells before discussing source, screening, and treatment goals with a qualified clinician.
How collection, comfort, and recovery differ
Where the cells come from
The clearest difference between bone marrow aspirate and umbilical cord stem cells is who provides the source material. Bone marrow aspirate comes from the patient, so collection is part of the treatment process. Umbilical cord material comes from donated tissue collected after birth, before the patient arrives for care.
This difference changes the practical experience. A bone marrow plan includes both a collection procedure and the planned treatment. An umbilical cord plan does not require marrow collection from the patient. A scientific review describes postnatal umbilical cord tissue as a readily available cell source, but availability alone does not prove that it is right for every patient.
Comfort during treatment
Bone marrow aspiration is invasive and usually involves anesthesia. Patients should ask where aspiration will occur, what pain control is used, and how long collection may take. They should also ask whether the collection and treatment happen during the same visit. These details can shape comfort and the day’s schedule.
With donated umbilical cord sourcing, the patient does not undergo the harvest step. The clinical visit still depends on the planned route of treatment and the area being treated. An injection may cause discomfort even when no marrow is collected. A consultation should explain each step without suggesting that either option is painless or risk-free.
What recovery may involve
After bone marrow aspiration, recovery may involve both the collection area and the treatment area. This can affect plans for work, driving, exercise, and help at home. Before treatment, ask which activities to limit and when normal activity may resume. Also ask which symptoms require a call to the clinic.
An umbilical cord-based plan removes the need to recover from marrow collection. Recovery still varies with the treatment site, the patient’s health, and the care plan. Patients comparing umbilical cord stem cells with bone marrow aspirate should focus on the full visit, not only the cell source.
Neither collection method can promise a specific result or recovery time. A clear plan should cover preparation, comfort measures, aftercare, and follow-up before consent. It should also explain why the recommended source fits the patient’s goals and health history. That practical discussion helps patients compare options with realistic expectations.
Why patient age can matter for cell quality
The changing starting material
In an autologous bone marrow procedure, the collected cells come from the patient’s own body. That source avoids donor tissue, but the starting material is not the same for every patient. Age is one reason for this variation.
As people age, the yield and quality of cells collected from bone marrow may decline. The final bone marrow aspirate can therefore vary between younger and older patients. A clinician should also review the patient’s health, diagnosis, and treatment goals rather than use age alone.
A laboratory comparison of MSC sources found that umbilical cord blood MSCs had the highest cell growth and clonality rates. They also showed lower levels of several markers tied to cell aging than adult-source MSCs. These lab findings describe cell behavior, not a guaranteed patient outcome.
What a standardized profile means
Umbilical cord MSCs come from young donor tissue instead of a patient’s own marrow. This removes patient age as a feature of the harvested cells. It does not mean that every cord-derived product is identical or that cord cells are always the better choice.
A standardized profile means the source and processing criteria can be set before treatment. Collection, screening, handling, storage, and preparation still matter. Consistent production standards may reduce source variation, but they cannot ensure the same response for every patient.
Patients can review the source in more detail through this guide to umbilical cord stem cells. When comparing options, ask how the tissue was sourced, screened, processed, and stored. These details offer more useful context than the word “young” alone.
Age, potency, and treatment decisions
In the bone marrow aspirate vs umbilical cord stem cells discussion, potency needs a clear meaning. It may refer to cell count, growth in a lab, signaling activity, or another test. Those measures are related, but they do not automatically predict relief or improved function.
A careful comparison should separate cell-source features from expected clinical results. Both options require a review of the condition being treated and the available evidence. The treatment plan should also account for the patient’s health and tolerance for collection procedures.
- Ask what tests were used to assess cell identity, quality, and safety.
- Ask whether age or health could affect an autologous bone marrow collection.
- Ask how cord tissue donors and finished products are screened.
- Discuss realistic goals, limits, and follow-up before choosing a cell source.
Age can help explain why autologous marrow varies, while young donor tissue offers a more controlled starting point. It is one part of the decision, not proof that one source will produce a better result.
Are umbilical cord stem cells immune privileged?
Umbilical cord-derived mesenchymal stem cells (MSCs) are often described as immune privileged because they tend to prompt a limited immune response. Still, that term can be misleading. These cells are not invisible to the immune system, and immune privilege does not make every product or treatment suitable for every patient.
Lower immunogenicity, not zero risk
MSCs can interact with immune signals and may help regulate inflammation. Research comparing MSCs from umbilical cord blood, bone marrow, and fat found similar immunosuppressive activity across these sources. The same laboratory comparison of MSC sources found that cord blood-derived MSCs had the highest rates of cell growth and clonality.
Lower immunogenicity can support allogeneic use, which means cells come from a donor rather than the patient receiving them. Yet an allogeneic product can still cause an immune response. Source tissue, processing methods, cell condition, dose, and the patient’s health may all shape that response.
Screening and matching considerations
Donor screening and product testing remain important even when MSCs have low immunogenicity. Screening looks for concerns such as transmissible infections and problems with the source material. Product checks may assess identity, purity, sterility, and cell condition before use.
Matching needs also depend on the cell product and its planned use. The process is not always the same as matching for a cord blood transplant. Readers comparing cord sources can review the difference between cord blood vs tissue stem cells, since the terms describe distinct materials.
Why a physician reviews each case
A physician still needs to assess the patient before recommending an allogeneic cell-based approach. That review may cover immune conditions, current medicines, prior reactions, infection risk, treatment goals, and the available evidence. It also helps distinguish a careful clinical plan from a broad claim based only on the words “immune privileged.”
In this treatment discussion, immune response is only one part of the choice. Bone marrow aspirate uses the patient’s own cells, while cord-derived cells come from screened donor tissue. A review of umbilical cord stem cells can help patients prepare more focused questions for their physician.
BMAC vs Wharton’s Jelly stem cells: what changes clinically?
When comparing bone marrow aspirate vs umbilical cord stem cells, the first clinical difference is the source. Bone marrow aspirate concentrate, or BMAC, starts with marrow collected from the patient. Wharton’s Jelly comes from donated umbilical cord tissue and contains MSCs and cell-signaling factors.
These are not simply two names for the same material. Source, collection, processing, and patient health can all shape the treatment plan. The differences also affect what happens before the planned injection or other regenerative procedure.
Collection and preparation
BMAC requires a separate marrow collection step before treatment. The clinician aspirates marrow, often from the pelvis, and then concentrates the sample. Because bone marrow aspiration is invasive and may require anesthesia, the protocol must account for collection-site care and added recovery needs.
Wharton’s Jelly does not require marrow collection from the person receiving treatment. This can simplify the visit and avoid discomfort at a marrow collection site. Patients researching cord blood vs tissue stem cells should also note that Wharton’s Jelly is cord tissue, not cord blood.
- BMAC is autologous, meaning the starting marrow comes from the patient.
- Wharton’s Jelly is sourced from donated umbilical cord tissue.
- BMAC adds aspiration and concentration steps to the treatment day.
- Wharton’s Jelly preparation depends on the selected product and its handling protocol.
Cell source and signaling activity
MSCs from different tissue sources share several basic traits, but they are not biologically identical. A comparative study found similar surface markers, immune effects, and differentiation ability across several MSC sources. It also found that umbilical cord blood-derived MSCs had the highest proliferation and clonality rates.
The same MSC source comparison describes paracrine signaling as a main mode of MSC action. In simple terms, released signals may help shape nearby cell activity. These findings support careful source selection, but they do not prove that one source is best for every patient.
Practical protocol decisions
The clinical choice should begin with the treatment goal, the target tissue, and the patient’s health. BMAC may suit a plan that calls for the patient’s own concentrated marrow. Yet age and overall health can affect the starting material, so clinicians must assess each case.
A Wharton’s Jelly protocol removes the marrow aspiration step and uses a prepared cord-tissue source. The care team still needs to review product records, handling, treatment route, and realistic expectations. Miami Stem Cell’s Stem Cell Therapy overview explains how regenerative options fit within a personalized, non-surgical care plan.
Which option is right for joint pain or chronic inflammation?
There is no single answer for every person comparing bone marrow aspirate vs umbilical cord stem cells. The right fit depends on the source of pain, overall health, treatment goals, and comfort with each procedure. A clinician should also review whether regenerative care fits the diagnosis before discussing a cell source.
Pain patterns and goals
Joint pain can stem from cartilage wear, a tendon injury, an old sports injury, or another health issue. Chronic inflammation may also involve several joints or affect the whole body. These differences matter because a focused joint problem calls for a different plan than broad, ongoing symptoms.
Define what progress would mean before choosing an option. One person may want less pain during daily walks. An athlete may care more about joint load, range of motion, and a safe return to training. A personalized joint regeneration review can connect those goals to exam findings and medical history.
Age, collection, and cell source
Bone marrow aspirate uses cells collected from the patient. This approach may appeal to someone who prefers an autologous source and accepts a separate collection step. The clinician should explain how collection works, what comfort measures are used, and what recovery may involve.
Age also deserves attention during the comparison. Cell features can differ by tissue source. Research found higher proliferation and clonality in umbilical cord blood MSCs than adult bone marrow MSCs. The same laboratory study of MSC sources found similar surface markers, immune effects, and differentiation ability across sources.
Umbilical cord options avoid collecting bone marrow from the patient. People who want to learn more about sourcing and possible uses can read this guide to umbilical cord stem cells. Source alone does not predict how one person will respond, so it should not replace a full clinical review.
Medical history and safety questions
A thorough review should cover the diagnosis, symptom length, prior injuries, past procedures, current medicines, and other health conditions. Tell the clinician about recent infections, immune concerns, bleeding issues, and any drugs or supplements you take. These details help the care team decide whether to proceed, adjust the plan, or suggest another path.
Ask where the cells come from, how they are screened and handled, and what is known about the proposed product. Also ask about procedure risks, expected discomfort, aftercare, activity limits, and signs that require a call. Clear answers should include realistic limits, not promised outcomes.
- For a single painful joint: ask how the diagnosis and injection target were confirmed.
- For chronic inflammation: ask whether another cause needs testing or care first.
- For sports injuries: ask how the plan fits rehabilitation and return-to-play goals.
- For older adults: ask how age, health, and cell source affect the decision.
The final choice should follow a medical exam and an open discussion of alternatives. It should reflect the patient’s goals, risk tolerance, and ability to follow aftercare. A careful plan may support function, but no responsible clinician can promise a specific result.
How a physician recommends a regenerative protocol
A regenerative protocol should follow a diagnosis, not a preferred product. The physician first studies the problem, your health, and the function you want to regain. That process helps frame the choice of bone marrow aspirate vs umbilical cord stem cells around your needs.
The consultation and assessment
A useful consultation starts with the cause, location, and effect of your symptoms. The physician also checks whether another condition or treatment could change the risks or likely response.
-
Review your health history, prior treatments, medicines, allergies, and current symptoms. Bring past records and note what helped, what failed, and why.
-
Complete a focused exam to assess pain, movement, strength, and function. Imaging or lab work may be ordered when it could clarify the diagnosis.
-
Confirm the likely diagnosis and whether regenerative care fits the problem. This step may also show that another type of care is more suitable.
-
Set practical goals, such as walking farther, returning to a sport, or easing pain during daily tasks. Clear goals give the follow-up visits something useful to measure.
-
Discuss the procedure, possible benefits, limits, risks, and other care choices. Bone marrow collection involves aspiration, while an umbilical cord option avoids collecting marrow from the patient.
-
Choose a cell source and delivery plan based on the diagnosis, health history, goals, and evidence. Research comparing MSC sources found similar core traits, while cord blood-derived MSCs showed higher proliferation and clonality.
-
Create an aftercare and follow-up schedule before treatment begins. The plan should explain activity limits, warning signs, supportive care, and when progress will be reviewed.
Risk and source discussion
No cell source is automatically right for every patient. A physician should explain why a source fits the diagnosis and how it affects collection, treatment, and recovery. Patients who want more background can review this guide to umbilical cord stem cells before the visit.
The discussion should also cover realistic limits. Regenerative care is designed to support healing and function, but the response can differ by person. Ask what evidence applies to your condition, which unknowns remain, and what would make the physician change the plan.
Aftercare and follow-up
Aftercare is part of the protocol, not an extra step. Written guidance should explain movement, exercise, other therapies, medicines, and symptoms that need a prompt call. Follow-up visits let the physician compare progress with the goals set during the first consultation.
If function does not improve as expected, the physician can review the diagnosis and adjust supportive care. Patients considering a personalized plan can schedule a consultation to discuss their records, goals, and suitable next steps.
Frequently Asked Questions
Are umbilical cord stem cells better than bone marrow stem cells?
Neither source is universally better. The right choice depends on the condition, treatment goal, health history, and evidence for the proposed use. Umbilical cord-derived MSCs showed higher proliferation and clonality in one laboratory comparison. However, those findings do not prove better patient outcomes. A qualified clinician should explain the evidence, risks, and regulatory status before treatment.
What stem cell source may be considered for joint pain?
The appropriate source for joint pain depends on the diagnosis, joint damage, age, health history, and available clinical evidence. In one retrospective knee study, both bone marrow aspirate concentrate and umbilical cord-derived MSC groups improved over follow-up, without statistically significant differences between them. These findings may not apply to every patient or treatment method, so an individual medical evaluation is essential.
Is surgery required for bone marrow stem cell collection?
Bone marrow collection requires an invasive aspiration procedure, usually from the pelvic bone. The area is typically numbed, and sedation or other anesthesia may be used depending on the setting. Collection can cause temporary pain, soreness, bruising, or bleeding. Umbilical cord-derived cells do not require marrow harvesting from the patient, which removes that additional collection procedure from the treatment process.
How does age affect the quality of bone marrow stem cells?
Bone marrow-derived cells come from the patient, so their characteristics may change with age and overall health. Research comparing MSC sources found that umbilical cord blood-derived MSCs had higher proliferation and lower expression of several senescence markers than adult bone marrow-derived MSCs. The study was laboratory-based, so it does not establish that one source produces better clinical outcomes for every patient.
Ready to compare your regenerative options?
Delaying a personalized evaluation can leave you managing the same concerns while uncertainty about the right regenerative approach continues. Starting now gives your medical team time to review your goals, health history, and treatment preferences before recommending a suitable path. An early conversation can also help you understand procedural differences, expected timelines, and practical next steps without committing to treatment.
Ready to compare your options with a qualified medical team? Schedule a free consultation to discuss whether bone marrow aspirate or umbilical cord stem cells may fit your needs. Schedule your free consultation to get personalized guidance and a clear plan for moving forward.